Manitoba registry
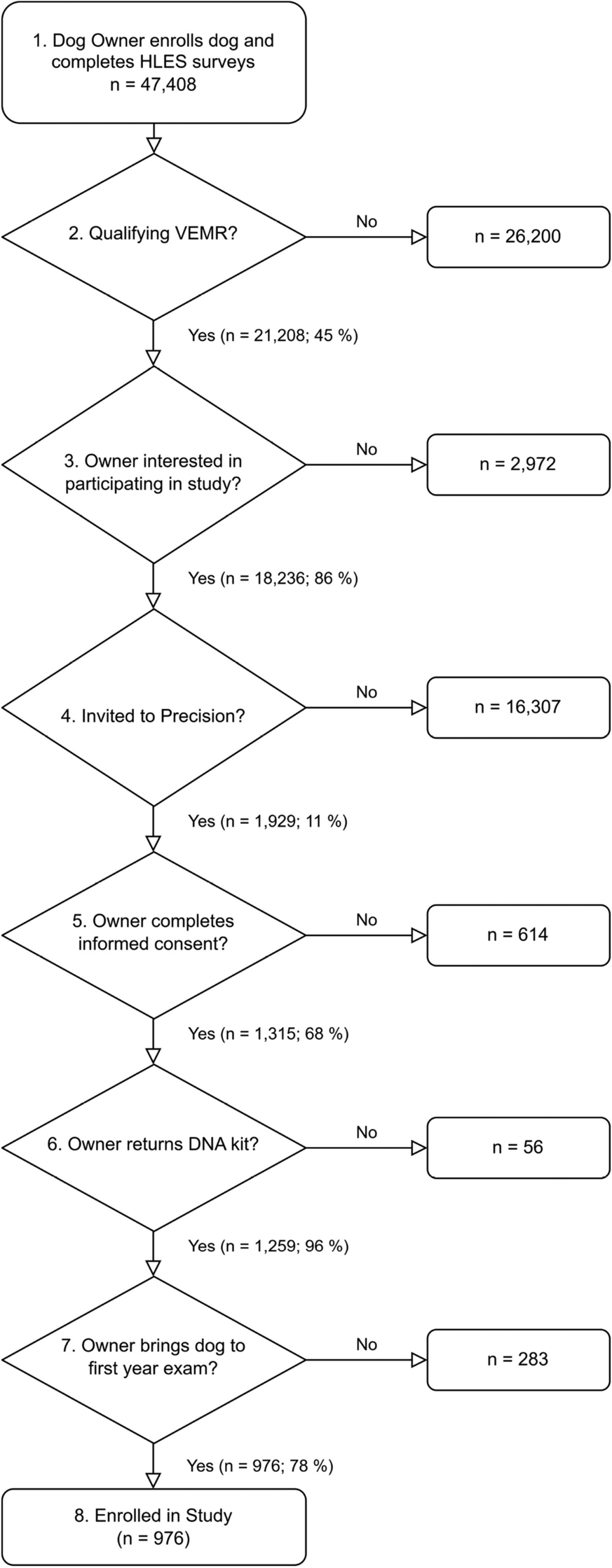
The Manitoba Bone Mineral Density Program manages all clinical DXA testing in the Province of Manitoba, Canada, and maintains a registry of all results. The Program includes VFA images in DXA assessment since 2010 for qualifying individuals using the criteria T-score of ≤ − 1.5 (minimum at the lumbar spine, total hip, or femoral neck) plus any of (a) age ≥ 70 years, (b) age 50 to 69 years and historical height loss (recalled young adult height minus current height) > 5 cm or measured height loss > 2.5 cm, or (c) glucocorticoid exposure for at least 3 months over the past year. All scans were performed using fan-beam DXA instruments (Lunar Prodigy or iDXA, GE Healthcare, Madison, WI). From the initial 13,395 de-identified VFA images obtained as part of osteoporosis assessment from February 2010 to December 2017, 4830 were excluded for various reasons (e.g. no linked health records, poor image quality, images from the same patient), as detailed in Supplementary Fig. 1. This left 8565 unique individuals with a VFA image where the ML-AAC24 algorithm was applied for inclusion into the current study.
AAC assessment and development
De-identified VFA images were available from two different models (Lunar Prodigy, iDXA) of bone density machines manufactured by GE Healthcare (Madison, WI). The ML-AAC24 scores were developed based on the Kaupilla AAC24 [23] semi-quantitative scoring method undertaken by an expert and described in detail previously [21]. To manually score AAC24, the posterior and anterior walls of the abdominal aorta are divided into four segments each, corresponding to the spaces anterior to vertebral levels L1, L2, L3, and L4. Within these eight segments, the AAC score was assigned as follows: 0 if no calcification was observed, 1 if less than one third of the aortic wall length in that segment was calcified, 2 if one third or more but less than two-thirds of the aortic wall length was calcified, and 3 if two-thirds or more of the aortic wall length was calcified. The total AAC score, ranging from 0 to 24, is calculated as the sum of the scores from the eight segments. The AAC24 scoring method is the most used method with higher intra-rater reliability (intraclass correlations coefficients (ICC) above 0.9) compared to AAC-8 scoring (ICC 0.8–0.9) [23, 24]. Expert scores served as the ground truth for the ML-AAC24 algorithm training (n = 2590) [21]. Specifically, the ML-AAC24 algorithm was developed on a randomly chosen subset comprising 90% of images (n = 2331) of those with expert AAC readings, and subsequently, it was tested on an additional 10% of images (n = 259). This process was iterated through tenfold cross-validation to predict AAC scores for each 10% random sample (n = 259). The intraclass correlations between expert and ML-AAC24 readings were 0.90 and 0.79 for VFA images acquired using iDXA and Lunar Prodigy DXA machines, respectively. Similar to previous reports on AAC classification based on severity [12, 21], ML-AAC24 was categorised as low (ML-AAC24 < 2), moderate (ML-AAC24 ≥ 2 to < 6), and high (ML-AAC24 ≥ 6). The performance of ML-AAC24 to classify individuals into the three ML-AAC24 severity groups was detailed previously [21]. Specifically, average classification accuracy (76.6%), sensitivity (60.4%), specificity (81.9%), negative (81.9%), and positive (63.0%) predictive values were acceptable for the Lunar Prodigy. For the iDXA, average classification accuracy (85.0%), sensitivity (74.2%), specificity (88.8%), negative (88.9%), and positive (74.0%) predictive value were better.
The final algorithm, which is an ensemble of ten convolutional neural networks derived from the aforementioned subsets, was then applied to estimate ML-AAC24 for 8565 VFAs (without expert readings or used in the development of the algorithm) for inclusion in the current study.
Fall-associated hospitalisation
The primary outcome for this study was fall-associated hospitalisation after VFA (index date) up until the 31st of March 2018. We also identified individuals with a prior fall using a look back of fall-associated hospitalisation diagnoses or self-reported falls that occurred in the 12 months prior to the index date. Data for incident fall-associated hospitalisations were based upon hospital discharge abstract codes ((ICD-9-CM) prior to 2004 and International Classification of Diseases, 10th Revision, Canadian Enhancements (ICD-10-CA)). Fall codes included E880–886, 888 for ICD-9-CM, and W00-W19 for ICD-10-CA. Incident fall-associated hospitalisations were assessed from routine prospectively collected linked administrative data, independent of self-report.
Baseline characteristics
Multiple covariates that could contribute to CVD and musculoskeletal health were identified and included in the adjusted models. This included age, sex, body mass index (BMI), current tobacco smoking, high alcohol intake (3 or more drinks per day) assessed at the time of VFA, diagnoses of diabetes, chronic kidney disease (CKD) hypertension in the last 3 years (linked physician claims and hospitalisation records), and prior myocardial infarction or cerebrovascular disease at any time since 1984 (linked hospitalisation records). Social determinants related to income (lower two quintiles versus upper three quintiles), area of residence (rural versus urban), and ethnicity (self-reported white versus non-white) were also included [25, 26]. Medications used for at least 6 months in the year prior to the index date were identified from the province-wide retail pharmacy database (use of any spironolactone, glucocorticoid, statin, nonselective beta blocker, selective beta blocker, angiotensin receptor blocker, ACE inhibitor, aldosterone blocker, loop diuretic, thiazide diuretic, digoxin, calcium channel blocker, long-acting nitrate, diabetes medications, oral anticoagulant) [27, 28].
Statistical analysis
Kaplan–Meier survival analysis was used to determine the relationship of ML-AAC24 categories (low, moderate, and high) with incident fall-associated hospitalisations. This relationship was further examined using multivariable-adjusted Cox proportional hazards models. Three models of adjustment were included: Model 1 adjusted for age and sex; Model 2 adjusted for Model 1 plus BMI, tobacco use, high alcohol intake, income, rural residence, ethnicity, diagnoses of diabetes, hypertension, and medication use in the prior year (glucocorticoid, statin, nonselective beta blocker, selective beta blocker, angiotensin receptor blocker, ACE inhibitor, aldosterone blocker, loop diuretic, thiazide diuretic, digoxin, calcium channel blocker, long-acting nitrate, and oral anticoagulant); and Model 3: Model 2 plus prior falls in the last year. The proportional hazards assumption was confirmed from graphical analyses and Schoenfeld residuals. The log-likelihood chi-square statistic was used to evaluate the significance of removing individual predictor variables from the multivariable-adjusted analysis (Model 3). The resulting change in log-likelihood chi-square for each predictor variable was used for ranking its relative importance in relation to falls. A larger change in log-likelihood chi-square upon the removal of a variable from the final model indicates a variable of greater importance. All analyses were performed using IBM SPSS (Version 27; IBM Corp., Armonk, NY, USA).
Sensitivity analyses
As lower BMD [29] and CVD [9] have been linked to increased fall risk, we further adjusted the primary analysis for hip BMD as well as prior major CVD, comprising myocardial infarction (ICD-9-CM 410, ICD-10-CA I21) or cerebrovascular disease (ICD-9-CM 433–435, ICD-10-CA I63-66, G45) from linked health records since 1984. As diabetes medications and CKD can influence vascular calcification [16], these variables were also added as covariates to Model 3 when examining the relationship between ML-AAC24 categories and fall-associated hospitalisations. As individuals with prior falls likely have a much higher fall risk, which could bias our results, further analysis excluding these prior fallers (n = 1332) as part of the primary analysis between ML-AAC24 categories and fall-associated hospitalisations was undertaken. Although the proportion of males in this study was low (6.0%), we undertook exploratory sex-specific analysis, including interaction testing (sex*ML-AAC24 categories), to determine if the relationship between ML-AAC24 and fall-associated hospitalisations was influenced by sex.



Comments (0)