Comprehensive genomic profiling (CGP) can only be used in patients with advanced solid tumors who have completed standard chemotherapy or who lack appropriate standard chemotherapy options. The CGP results were explained to the patient by their physician after review by an Expert Panel (EP). Clinical and genetic mutation data obtained through CGP were provided to the C-CAT with patient consent. In Japan, two tissue-based CGP tests, Foundation One® CDx (F1CDx) and OncoGuide™ NCC Oncopanel (NCC Oncopanel), became reimbursable under the National Health Insurance Scheme administered by the Ministry of Health, Labour, and Welfare in Japan in June 2019. Additionally, liquid-based Foundation One® Liquid CDx was covered in 2021. Moreover, the liquid-based Guardant360 and tissue-based GenMine Top Panel were covered in June 2023. The CGP results and clinical data from nearly all patients who underwent CGP testing were collected from the C-CAT [13]. The study used data from patients with breast cancer who consented to both data registration with the C-CAT and secondary use of their data.
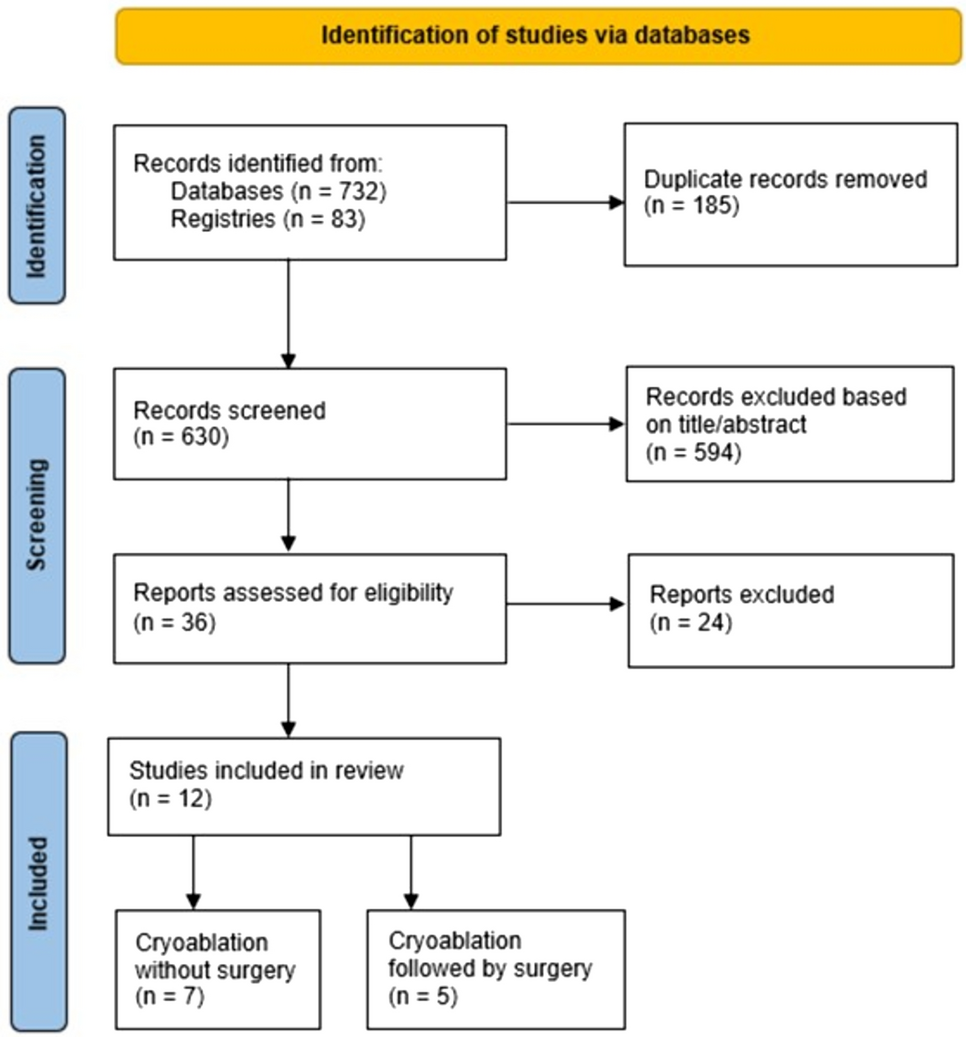
From June 2019 to February 2024, C-CAT included 4084 mBC cases with annotated genomic profiles Among these, 1967 were classified as luminal-type breast cancer, characterized by estrogen receptor (ER) positive and/or progesterone receptor (PgR) positive, and HER2 negative (C-CAT Ver. 20240219). A flow diagram is shown in Supplementary Fig. 1.
Clinical data collected included patient age, sex, histological subtype, CGP testing type, post-CGP treatment, date of diagnosis and last observation, and survival status at the last observation. Data on annotated genetic alterations were collected using the C-CAT-provided OncoKB, ClinVar, and Cancer Knowledge databases. Gene alterations in the pathogenic or possibly pathogenic AKT pathways-altered (PIK3CA, AKT1, or PTEN) were extracted from this database.
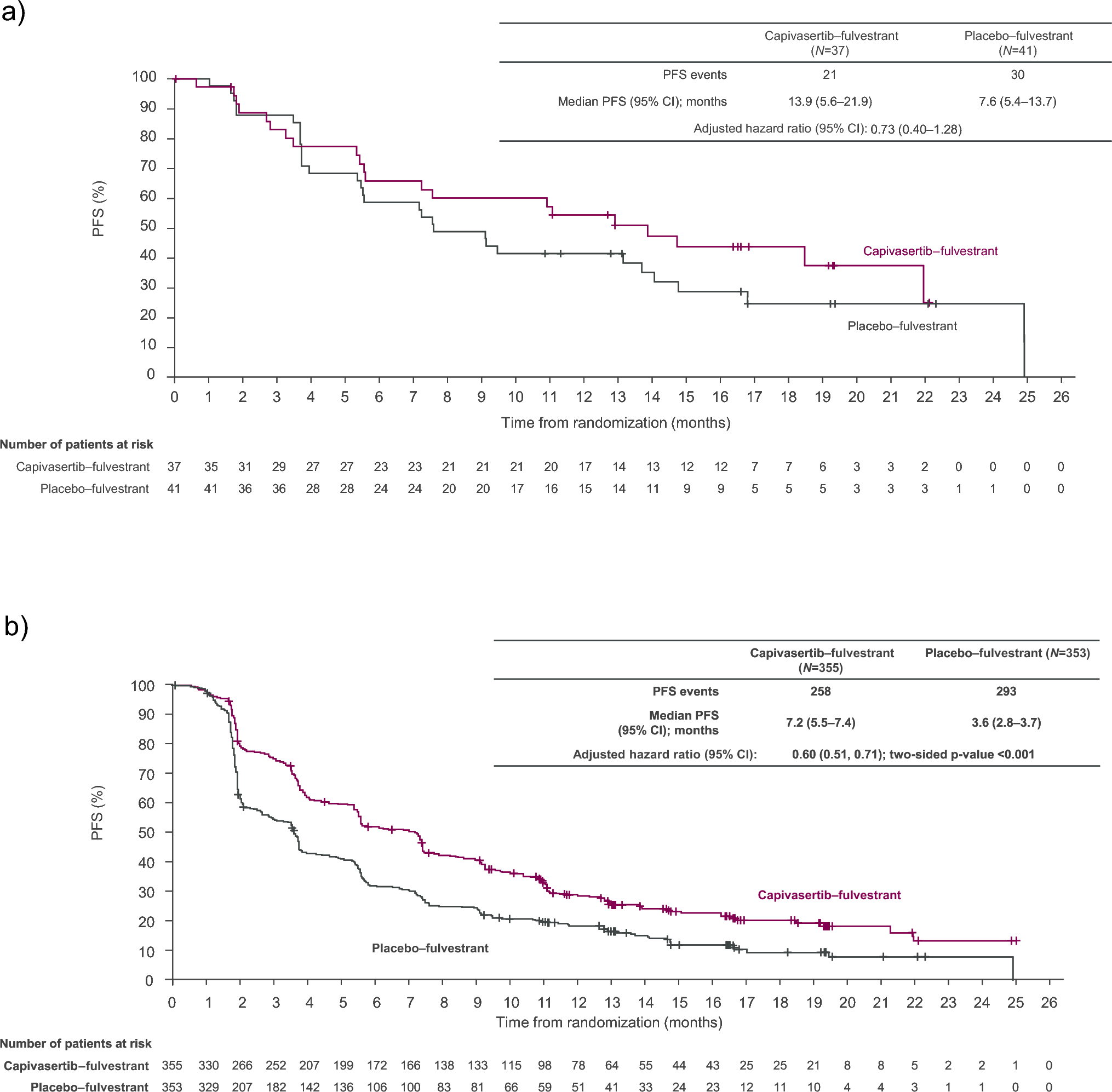
The companion diagnostic genes for capivasertib were based on CAPItello-291, with only E17K for AKT1 and 19 short variants of PIK3CA (R88Q, N345K, C420R, E542K, E545A, E545D, E545Q, E545K, E545G, Q546E, Q546K, Q546R, Q546P, M1043V, M1043I, H1047Y, H1047R, H1047L, and G1049R). PTEN included 13 short variants (C124R, C124S, G129E, G129V, G129R, R130Q, R130G, R130L, R130P, C136R, C136Y, S170R, and R173C) and any nonsense, frameshift, or splice site alterations. PTEN rearrangement was assumed to be a homozygous deletion of one or more exons, or any event that disrupts protein function, such as intragenic events (duplications of only part of the gene, deletions, inversions, and translocations) regardless of the transcript. Capivasertib companion diagnostic (CDx) genes were defined accordingly. Alterations of AKT1, PIK3CA, and PTEN other than the capivasertib companion gene were defined as non-CAPI CDx.
High tumor mutational burden (TMB) was defined as having at least 10 mutations per megabase (Mb) in the tissue-based panel and at least 14 in the liquid-based panel.
Cases involved individuals who had previously undergone germline BRCA1/2 testing with negative results, but the panel test demonstrated somatic BRCA1/2 gene alterations.
Based on the mutation data, the gene mutation profile was visualized using the OncoPrinter platform on cbiportal.org (accessed on June 11, 2024).
Statistical analysis was performed using R and its command input platform ezR [14]. Categorical variables were compared using the χ 2 test or Fisher’s direct probability test.
The study was approved by the Ethics Committee of Tohoku University Graduate School of Medicine (permission no. 2021-1-681) and the C-CAT Data Access Review Committee (CDU2022-008E03).



Comments (0)