
Remember me

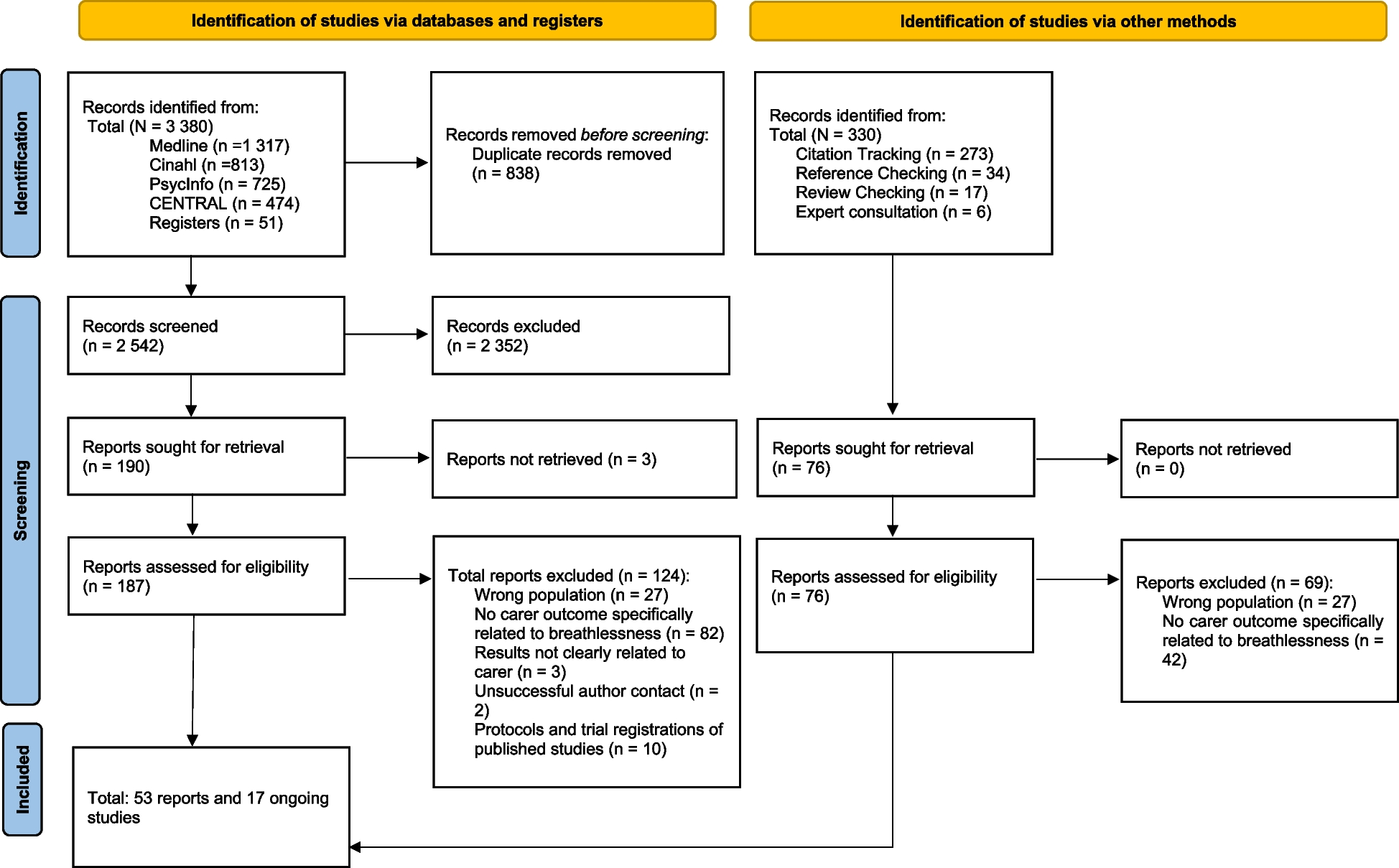








Our search until July 2023 retrieved 3,380 reports from databases and trial registers (see Fig. 1). Additionally, 330 reports were identified via forward and backward search. A total of 53 reports were included in the review. Seventeen ongoing studies were placed on the ‘awaiting classification’ list, none of them could be included during the project time (see Supplement III).
Of the 53 studies, we identified 20 qualitative studies (see Table 2) with a total of 217 carers, with samples ranging from four to 25 participants aged between 20 and 84 years, on average 59.5 years. The studies included one focus group [29] and 19 (two reports from one study) interview reports [14, 17, 29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46] as well as one published letter to the editor with qualitative interview data [47].
Table 2 Qualitative StudiesIn addition, we identified 32 quantitative studies (see Table 3 and Supplement V) with a total sample of 4,632 carers and sample ranges from three up to 670 carers. The average carers’ age was 63.6 years, ranged from 28 up to 73.4 years.
Table 3 Outcomes of quantitative studiesWe included 17 cross-sectional reports [13, 48, 49, 51,52,53,54,55, 57,58,59,60,61, 64, 66,67,68], two publications from one study population [59, 60], five mixed-method studies [69,70,71,72,73], with two publication from one study, three randomised (controlled) trials [74,75,76], one prospective study [56], two retrospective studies [62, 77], one economic study [65], three secondary analyses [50, 63, 78] based on two prospective observational cohort studies [50, 63] and one randomised controlled trial with data from the intervention arm [78] (see Table 4: RCTs and mixed-method studies).
Table 4 RCTs and mixed-method studiesThe most common underlying disease of the breathless patients was COPD (26 studies) followed by cancer (18 studies). Others were interstitial lung diseases, heart failure, amyotrophic lateral sclerosis, motor neurone diseases and silicosis. The majority of carers were female, only two studies reported more males [37, 55]. Studies were from 20 different countries, most from UK (n = 8), USA (n = 6), Canada (n = 5), Germany (n = 5), Australia (n = 3). The overall quality score (see Supplement IV) e.g. the mean score was 72% (± 20%) over all reports.
Findings of included studiesTo answer our review question, we structured the results using a theoretical framework that we developed for this purpose (see Fig. 2: Caregiving process), with four main categories: burden, (unmet) needs, coping strategies and the use of healthcare and social services. For each category, we first reported qualitative studies, then the quantitative ones, and finally an integration of both types of studies. A synthetic overview of the key findings is presented in Fig. 3.
Fig. 2 Fig. 3
Fig. 3
Overview of qualitative and quantitative findings
BurdenQualitative studies have reported an emotional burden on carers. Frequently mentioned were feelings of insecurity and fear related to the patient’s breathlessness as well as the carers´ uncertain future. A general uncertainty was a prominent theme in all studies. The sudden appearance of breathlessness and its unpredictability were both the cause and effect of a permanent state of uncertainty and alertness for carers [17, 29,30,31,32,33, 35, 37, 39, 40, 45, 46, 67]. Carers also suffered from severe sleep disorders and constant fear of their patient’s sudden death due to breathlessness, especially at night [30, 32, 33]. Inherent uncertainty due to anxiety and fear enormously increased the burden on carers.
I’d like somebody to tell me when it’s gonna happen. It’s like living with a pressure cooker or a time bomb. […] I know what his problems are. […] Although Mr. Johns told us it wouldn’t improve his breathing and everything like that, the build-up towards the operation was horrendous. (Carer of a patient with heart failure; Gysels et al. 2009, P. 155)
They were in a constant state of alertness and described patient’s breathlessness as a ‘frightening, little known, and poorly understood symptom’ [34] causing ‘primal distress’ [36]. Carers felt helpless and panicked because of a lack of knowledge about breathlessness and professional support structures [29, 31,32,33, 35, 36, 38,39,40,41]. As the following quotation highlights:
I thought he’d gone … it was terrifying really, it really is … you just don’t know what to do, you can’t do anything any way … you’re just helpless aren’t you. (Wife of emphysema patient aged 77, Interview; Booth et al. 2003, P. 341)
In addition, participants reported negative emotions owing to a lack of treatment interventions for their patients. Carers also reported a strong fear of being the trigger for patients´ next episode of breathlessness, e.g. through arguments, which may upset the patient and consequently cause breathlessness. This might result in emotional withdrawal and feelings of guilt among the carers [29, 32, 39, 44]. Therapeutic options such as oxygen therapy were identified as life-saving, but the carers felt burdened by the responsibility of determining the correct dosage for breathlessness relief and the underlying disease [36]. Nevertheless, when patients took opioids to reduce breathlessness, carers felt less stressed and noted an improvement in their own quality of life [44].
Four qualitative studies demonstrated how the relationship between carers and patients had evolved from a loving partnership to a new type of relationship with a new form of intimacy in the form of physical care and mutual dependence [34, 37, 39, 41].
I do not love him as I did earlier … I would rather say that I care immensely about him. This is more like fondness and friendship. (Participant 2; Bergs et al. 2002, P. 617)
Carers’ social lives were also more limited because of patients’ symptom deterioration [34]. Breathlessness was stated as the leading symptom among all diseases to a ‘shrinking world’ [32] and a major threat to care that intensified other symptoms and was the worst to handle [40]. Physical care, sleep disturbances, and carers’ health problems were further burdens. Additional challenges for carers due to the patient's underlying illness and breathlessness were limitations such as lack of barrier-free access to buildings to minimize patients´ physical burden, and the lack of visibility of patients´ underlying disease turned out to be a challenge in the consideration by others [17, 31, 35, 37]. Breathlessness required carer´s constant presence and created a strong mutual dependence and mutual suffering [41]. Breathlessness triggered dyadic anxiety or both patient and carers’ anxiety [17]. The following quotation describes this:
The first few times I called an ambulance, it was simply panic … although he was gasping for breath…he calms down the minute I phone an ambulance … It’s visible, because he knows and I know help’s on its way. (Carer 221; COPD; Farquhar et al. 2017, P. 7)
Carers also perceived a lack of problem awareness among healthcare professionals. They mentioned receiving little therapeutic advice to cope with breathlessness and having no access to support services (e.g., nursing) [17].
Seven quantitative cross-sectional studies [13, 48, 49, 51,52,53,54] and one prospective cohort study [
Comments (0)