
Remember me









Mathematics can assist us in understanding the mechanism of the cardiac motion and blood flow directions inside the heart [15,16,17,18]. In this regard, MATLAB software is very helpful for calculating and showing the velocity vectors of the LV myocardial samples using motion and deformation echocardiographic data.
In this study, patients hospitalized due to COVID-19 underwent 2D echocardiography examinations.
COVID-19 infection causes a complex interplay of inflammation-related factors such as von Willebrand factor and coagulation factor VIII release, complement activation, and fibrinogen increase, as well as cytokine storm, along with reduced endothelial anti-thrombogenicity due to vascular injury. These factors cause a decrease in blood flow in arteries, veins, and capillaries and lead to thrombus formation. On the other hand, there is a fact that without conditions such as hyper-eosinophilic syndrome (Loffler) or a severe decrease in ejection fraction or wall motion abnormality due to myocardial infarction or primary blood disorders, the formation of clots in different origins of the heart is sporadic. So we went to explore other causes for this phenomenon.
We included patients with normal noninvasive cardio-vascular diagnostic tests and normal myocardial motion in echocardiography and biochemical examinations but with a mass in their left ventricle, for example, in the apex of the heart or in the base of the intraventricular septum area in the study. All included patients were treated with anticoagulant agents during hospitalization, and the masses disappeared within days, which thus supports that the masses were most likely clots. The motion and deformation echocardiographic data were imported into MATLAB software to display the velocity vectors of the blood inside the left ventricle.
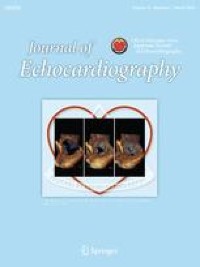
In normal cases, blood flows inside the left ventricle through the mitral valve, hits the lateral LV-free wall, experiences clockwise turbulences at the apex, hits the septal wall, and flows toward the aortic valve (Fig. 1A–D) [19,20,21]. Analyzing these data using the MATLAB program, we determined that in the rapid filling phase of a normal heart, blood flow inside the left ventricle is irrotational. Conversely, blood moves rotationally in a clockwise direction at the diastasis phase and irrotationally in the late filling phase. This is followed by the early IVC period, during which the blood flow travels rotationally in a counterclockwise direction. In the same way, the vortex located in the proximity of the anterior mitral leaflet in the LV outflow tract (LVOT) region moves in a counterclockwise direction. During the late IVC period, the vortex remains in the LVOT region, and its direction is toward the aortic valves (Fig. 1A–D and Video 5) [22].
Fig. 1
Blood circulation in a normal heart left ventricle: A the rapid filling phase has an irrational flow shown by green velocity vectors. B Blood as a fluid moves rotationally in a clockwise direction at the diastasis phase. C In the late filling phase, blood has an irrational flow (a non-rotational bunch velocity vectors) obscuring the vortex. D In the early iso-volumic contraction (IVC) period, the blood flow has a counterclockwise rotation. During the late IVC phase and ejection time, the vortex remains in the LVOT region, and the blood flows directly toward aortic valves
Based on previous studies, it seems that the direction of blood flow in healthy people and normal cases follows a common pattern [22].
However, in our cases, we observed that whenever the blood fluid entered the left ventricle, it demonstrated a rotational flow during the rapid filling phase and then moved in a straight direction during the diastasis phase. This reversal of flow direction might be a main reason for clot formation at the apex of the heart. However, the rotational flow was observed again in the late filling phase, followed by the early IVC period, where the blood flow traveled rotationally in a clockwise direction toward the LV-free wall (Figs. 2, 3, 4, Videos 3 and 4). We also observed a delay, which means a slower blood flow inside the left ventricle compared to the normal heart phase. These abnormal flow directions could be a potential etiology for clot formation in the intraventricular septum area.
Fig. 2
Blood flow circulation inside the left ventricular cavity of a COVID-19 patient with an apical clot (patient number 8): A green velocity vectors show the blood flow during the rapid filling phase and are rotational. B Blood fluid moves in a straight direction at the diastasis phase. C In the late filling phase, the blood flow has a rotational flow again. D In the early iso-volumic contraction (IVC) period, the blood flow has a clockwise rotation toward the LV-free wall
Fig. 3
Blood flow direction inside the left ventricular cavity of the same COVID-19 patient (patient number 8) after the clot resolves with anticoagulation therapy is the same as when the clot is present, with the difference that the delay in the direction of the blood flow is reduced. A Green velocity vectors show the blood flow during the rapid filling phase and are rotational. B Blood fluid moves in a straight direction at the diastasis phase. C In the late filling phase, the blood flow has a rotational flow again. D In the early iso-volumic contraction (IVC) period, the blood flow has a clockwise rotation toward the LV-free wall
Fig. 4
Blood flow circulation inside the left ventricular cavity of a COVID-19 patient with a clot in the base of the interventricular septum (patient number 10): A in these transesophageal echocardiography views, green velocity vectors located under the mitral valve during the rapid filling phase have a rotational flow. B A bundle of green velocity vectors moves non-rotationally at the diastasis phase. C In the late atrial contraction time, the blood fluid had a rotational flow again and inclined toward the left ventricle's free wall. D In the early iso-volumic contraction (IVC) period, the blood flow has a clockwise rotation toward the LV-free wall
The anomalous blood trajectories inside the LV cavity suggest that cardiac wall motion in COVID-19 patients is not satisfactorily able to circulate the blood fluid in normal directions. However, regardless of the normal myocardial motion in our patients, what causes this abnormal blood flow?
COVID-19 is an acute infectious disease, and according to Sloop et al. [12], both acute and chronic inflammation exhibit the potential to increase blood viscosity. Because blood is a non-Newtonian fluid (as its viscosity varies with its shear rate), the increase in blood viscosity (caused by inflammation) in low-shear conditions can increase the risk of thrombosis on its own. Conversely, an increase in blood viscosity can lead to an increase in weight and pressure per unit area inside the heart, a decrease in kinetic energy, and an increase in inertial energy. These changes might cause the inability of the normal myocardium to lead the blood in its correct direction during a cardiac cycle and thus change the blood flow vectors inside the heart cavities (Figs. 2A–D, 3A–D and Videos 3 and 4) [23,24,25]. Based on these findings, the behavior of the blood inside the LV of COVID-19 patients is more like an abnormal Newtonian fluid (Figs. 2, 3, 4). The delay (slower blood flow inside the left ventricle) can be due to the abnormal blood flow direction and/or the increased viscosity of blood, which creates a force in the opposite direction of the blood flow. This viscous force is something like friction that slows down the movement of blood fluid. The above-mentioned conditions can be considered as possible etiologies for the clots inside the heart cavities of COVID-19 patients with normal myocardial motion [26].
Since the blood inside the left ventricular cavity is in interaction with the myocardial muscle as a fluid, according to Newton's laws and Euler Lagrange's laws, changes in blood specification may cause changes in the myocardium, such as the myocardial wall thickening or abnormal changes in the movement of the ventricular myocardial wall in the long term. Proving this hypothesis requires a separate study on COVID-19 patients over an extended period.
Comments (0)