
Remember me
Lower extremity injuries are highly prevalent among young athletes, with female athletes often facing a 2–8 times higher non-contact anterior cruciate ligament (ACL) injury rate compared to male athletes (Wild et al., 2012). Exercise-based interventions represent a comprehensive training approach that includes neuromuscular training, comprehensive warm-up exercises, core strength training, and specific balance training. These interventions aim to improve qualities such as strength, speed, agility, proprioception, and balance through targeted training. Currently, exercise-based preventive interventions have been widely applied in competitive sports, rehabilitation, and integrated into daily training as part of injury prevention programs (Johnson et al., 2020).
Multiple studies have demonstrated that exercise-based preventive interventions can reduce the incidence of lower extremity injuries and enhance athletic performance (Akerlund et al., 2020; Halvorsen et al., 2023; Pollard et al., 2017). However, some scholars argue that exercise-based preventive programs merely serve as pre-training warm-up routines and do not effectively prevent lower extremity injuries (Hilska et al., 2021). Consequently, there remains a certain degree of controversy regarding the effectiveness of exercise-based interventions. There remains a critical gap in understanding how the specific characteristics of these programs—duration, frequency, and intensity—affect their overall effectiveness. This gap signifies the need for a systematic evaluation that not only quantifies the impact of these variables on injury prevention but also identifies optimal program configurations for athletes across different sports. Furthermore, a consensus on the effectiveness of these interventions has not been reached.
The purpose of this meta-analysis is to identify Level 1 evidence studies on knee injury preventive interventions for athletes, evaluate the internal validity of these studies, and assess the quantitative effectiveness of these preventive programs. These interventions typically include a combination of neuromuscular, core strength, balance tailored specifically for athletes across diverse sports disciplines. The evaluation focuses on the duration, frequency, and intensity of these programs, aiming to quantitatively assess their effectiveness in reducing knee injury rates among athletes.
Materials and methodsSearch strategyThis review followed the 2020 guidelines of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA-ScR) checklist (Page et al., 2021) and was managed using Covidence online software. Electronic literature was systematically searched in English databases (PubMed, Web of Science, and EBSCO) and Chinese databases (CNKI and Wanfang Database) from January 1, 2000, to 12 April 2024, using key terms and their synonyms such as “Physical Activity, Sport, Training, Exercises, Acute Exercises, Aerobic Exercise, Isometric Exercise, Physical Exercise, prevent, reduces, Lower extremity injuries, Knee Injuries, Injury, Menisci, Medial Ligament of Knee, Anterior Cruciate Ligaments, Lateral collateral ligament, Cartilage, Patella, Kneecap” with the last search conducted on 12 April 2024, and all retrieved literature imported into Zotero for initial screening and further inclusion based on the PRISMA statement. The complete search strategy is provided in Supplementary Appendix A. The PICOS (patient, intervention, comparison, outcome, and study design) strategy and PRISMA checklist are provided in Supplementary Appendix A. Moreover, reference lists of included articles were also reviewed to ensure that all relevant studies meeting the selection criteria were identified.
Selection criteriaInclusion criteria①Study type: Randomized controlled trials (RCTs). ②Participants: Young athletes with sports experience. ③Information required: Sample size, gender, age of participants. ④Intervention: Additional or alternative interventions based on the original training program. ⑤Detailed experimental design and steps. ⑥Outcome measure: Number of lower extremity sports injuries. Lower extremity injuries include anterior and posterior cruciate ligament injuries, medial and lateral collateral ligament injuries, meniscus injuries, cartilage injuries, patellar injuries, etc.
Exclusion criteria①Non-randomized controlled trials, such as cohort studies. ②Review articles, animal studies, duplicate publications. ③Participants with existing diseases. ④Non-English or non-Chinese articles without full-text availability. ⑤Studies with poorly designed interventions and procedures. ⑥Studies with inconsistent outcome measures. ⑦Studies not meeting the inclusion criteria.
Data extractionTwo researchers conducted independent and blind extraction and data entry of relevant indicators from the finally included studies.
The extracted content included author and publication year, sample size, gender, age, intervention measures, number of injuries in the experimental and control groups, total number of participants, and intervention details (exercise time, weekly frequency, exercise period).
Quality assessmentCochrane Risk of Bias assessmentThe quality assessment of the included literature was performed using the Cochrane Risk of Bias assessment tool, which includes seven items: random sequence generation (A), allocation concealment (B), blinding of participants and personnel (C), blinding of outcome assessment (D), incomplete outcome data (E), selective reporting (F), and other biases (G) (Gu and Yang, 2014). Each item was scored as “yes,” “unclear,” or “no” for each article, with 1 point for “yes” and 0 points for “unclear” or “no.” Articles with a total score less than 3 were considered low-quality, 3 or 4 as moderate-quality, and 5 or more as high-quality.
Modified JADAD scaleThe included literature was assessed for quality using the modified JADAD scale (Jadad et al., 1996)), which includes four items: randomization (generation of random sequence), allocation concealment, blinding, and description of participant withdrawal or dropout details. Each item was scored as “appropriate,” “unclear,” or “inappropriate,” with 2 points for “appropriate,” 1 point for “unclear,” and 0 points for “inappropriate.” Scores of 1-3 indicated low-quality studies, while scores of 4–7 indicated high-quality studies.
Data analysis and processingReview Manager (Version 5.4, Cochrane) was used for the meta-analysis. Since the incidence of lower extremity injuries is a binary variable (injured vs. non-injured) in the experimental and control groups, the risk ratio (RR) and 95% confidence interval (CI) were used as the combined effect size. An RR value not including 1 and p < 0.05 indicates a statistically significant difference between groups. An RR = 1 indicates the same risk in the experimental and control groups, RR > 1 indicates a higher risk in the experimental group, and RR < 1 indicates a lower risk in the experimental group, with values closer to 0 indicating higher protection rates (Fu et al., 2016).The I2 statistic reflects the proportion of heterogeneity among the total variation in effect size and is commonly used to assess the degree of heterogeneity among studies. Low, moderate, and high levels of heterogeneity are represented by I2 values of 25%, 50%, and 75%, respectively (Wang et al., 2009). If I2 ≥ 50%, there is significant heterogeneity, and a random-effects model is used. If I2 < 50%, a fixed-effects model is used. Additionally, the heterogeneity test also includes the Q statistic, and if P < 0.1, it indicates significant between-group differences. Sensitivity and subgroup analyses are performed to identify the sources of heterogeneity. Publication bias is assessed using a funnel plot (Tang and Liu, 2000).
ResultsSearch outcomeThrough the search of the aforementioned databases, a total of 10,454 articles were retrieved, including 8,003 in English and 2,451 in Chinese. After excluding review articles, animal studies, and duplicate publications, 667 articles remained. Following the earlier mentioned inclusion and exclusion criteria, 119 articles that clearly did met the criteria were preliminarily screened in. After carefully reading the full texts and removing articles with inconsistent outcome measures and non-randomized controlled studies, 19 articles were included in the meta-analysis. The flowchart of the literature selection process is shown in Figure 1.
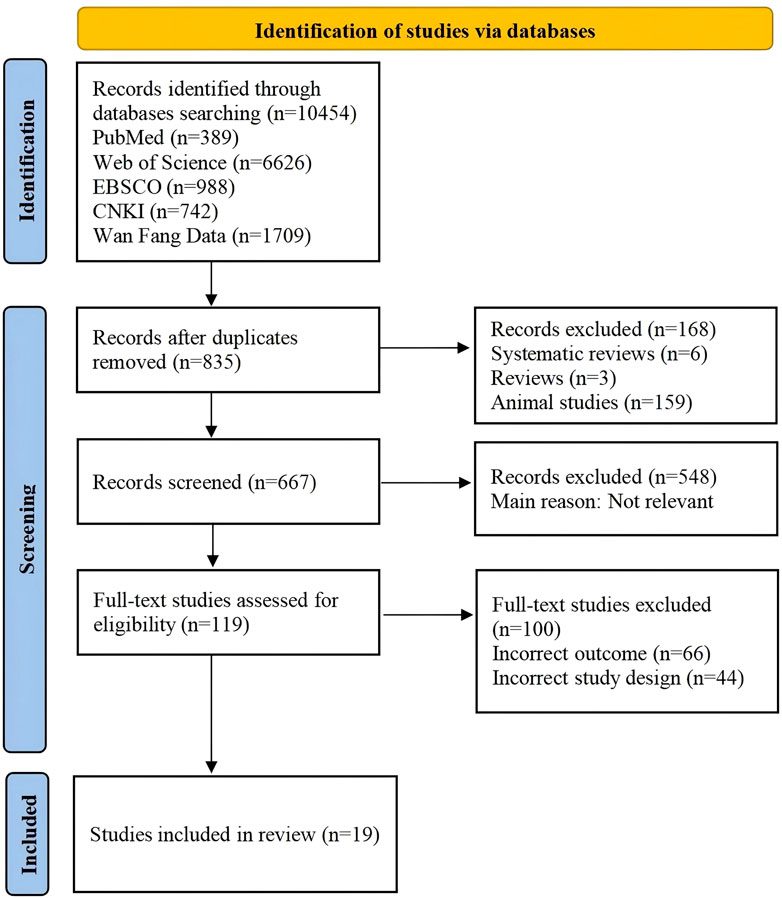
Figure 1. PRISMA flow chart..
Study characteristicsA total of 19 randomized controlled trials (RCTs) were included in the meta-analysis through rigorous inclusion and exclusion criteria (see Table 1). The ages of participants ranged from 12 to 26 years, with a higher proportion of female participants. The total sample size was 28,176 individuals. The sports disciplines covered in the interventions included basketball, volleyball, soccer, handball, and other team sports. The sports interventions encompassed proprioceptive training, neural control training, strength training, balance training, core stability training, and plyometric training. The range of exercise duration was 5–30 min per session, exercise frequency ranged from 1 to 5 times per week, and the exercise period ranged from 6 to 36 weeks.
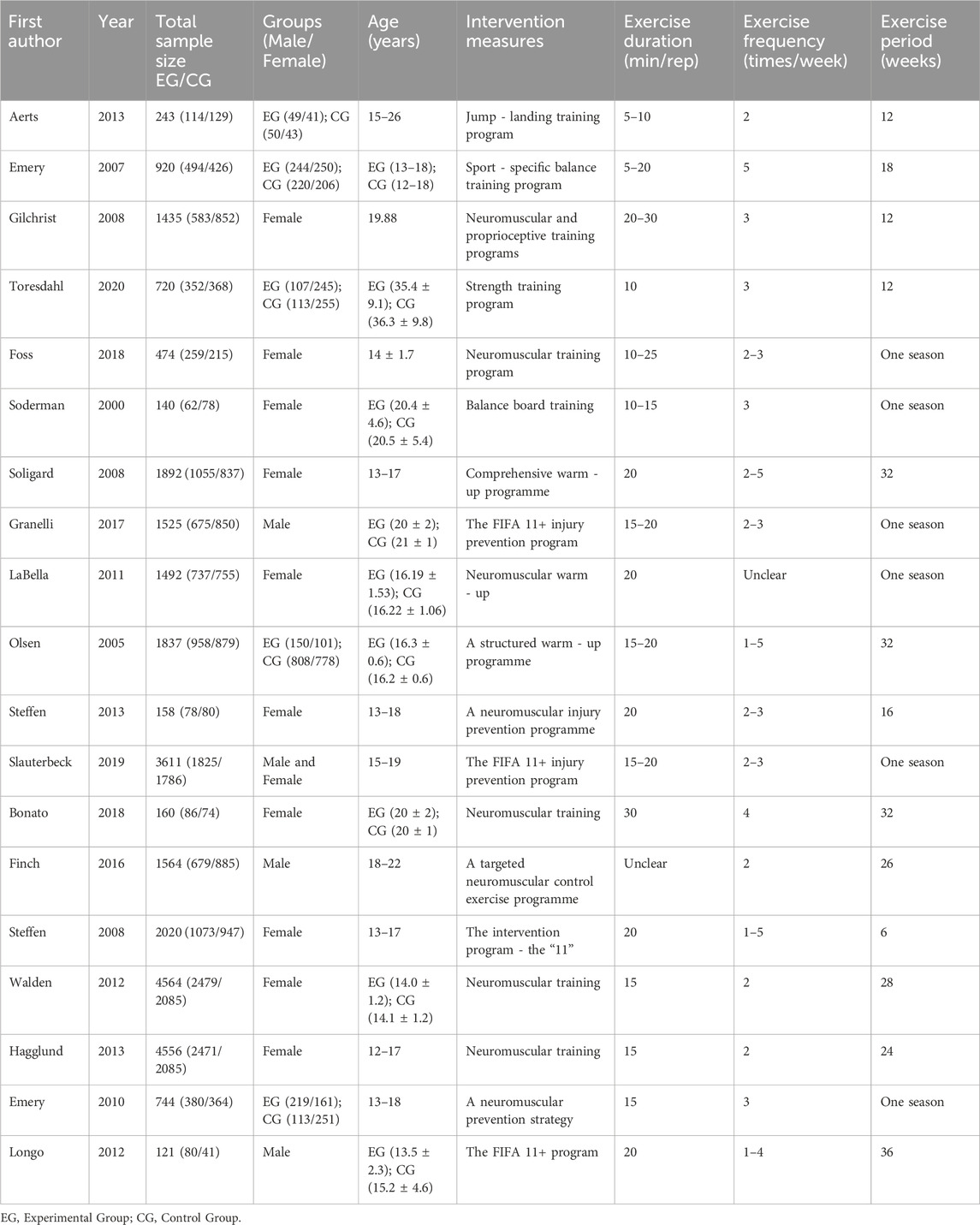
Table 1. Data extraction from included articles.
Evaluation of literature qualityCochrane Risk of Bias assessmentAll 19 included articles were randomized controlled trials. All articles reported the use of random sequence generation. Nine of these detailed specific methods such as random number generation, computer-generated randomization, or block randomization, suggesting a low risk of selection bias (Aerts et al., 2013; Bonato et al., 2018; Emery et al., 2007; Emery and Meeuwisse, 2010; Finch et al., 2016; LaBella et al., 2011; Longo et al., 2012; Silvers-Granelli et al., 2017; Walden et al., 2012). However, the remaining ten articles lacked detailed descriptions of their randomization process. Allocation concealment was not described in five articles (Foss et al., 2018; Gilchrist et al., 2008; Söderman et al., 2000; Toresdahl et al., 2020). Blinding of participants and personnel was adequately reported in three articles (low risk) (Bonato et al., 2018; Finch et al., 2016; Walden et al., 2012). Blinding of outcome assessment was reported in six articles (low risk), suggesting a thorough approach to reducing detection bias (Emery et al., 2007; Emery and Meeuwisse, 2010; Finch et al., 2016; Soligard et al., 2008; Steffen et al., 2013; Walden et al., 2012). The other 13 articles provided insufficient information on blinding of assessors (unclear risk). There were no incomplete data, selective reporting, or other biases identified, indicating a low risk in these domains. Based on the assessed criteria, 14 studies were deemed to be of high quality and five of moderate quality. The bias assessment results of the included articles are presented in Figures 2, 3.
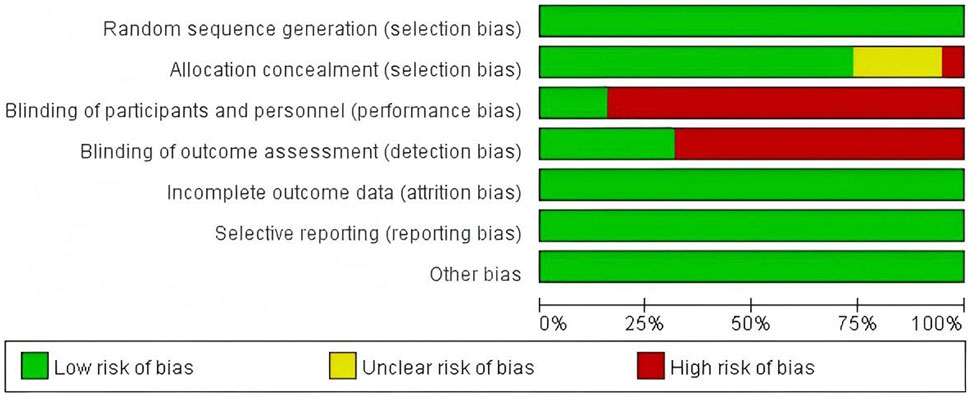
Figure 2. Risk of bias graph.
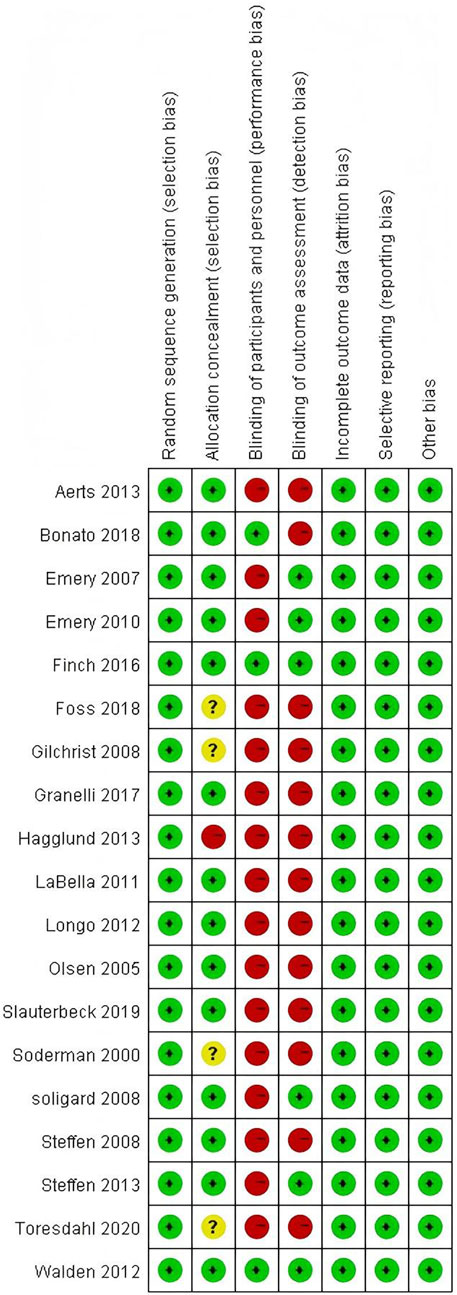
Figure 3. Risk of bias summary.
Modified JADAD scale score (double check results)Nine articles reported appropriate random sequence generation, scoring 2 points, while the allocation concealment was unclear in the remaining 11 articles, scoring 1 point. Fourteen articles mentioned allocation concealment, scoring 2 points, while the remaining 6 articles had unclear allocation concealment, scoring 1 point. One article mentioned double-blinding, scoring 1 point. All 19 articles described participant withdrawal or dropout details, scoring 1 point. Among the included studies, 14 were of high quality (Aerts et al., 2013; Bonato et al., 2018; Emery et al., 2007; Emery and Meeuwisse, 2010; Finch et al., 2016; LaBella et al., 2011; Longo et al., 2012; Olsen et al., 2005; Silvers-Granelli et al., 2017; Slauterbeck et al., 2019; Soligard et al., 2008; Steffen et al., 2008; 2013; Walden et al., 2012), and 5 were of low quality (Foss et al., 2018; Gilchrist et al., 2008; Hagglund et al., 2013; Söderman et al., 2000; Toresdahl et al., 2020). Refer to Table 2 for details.
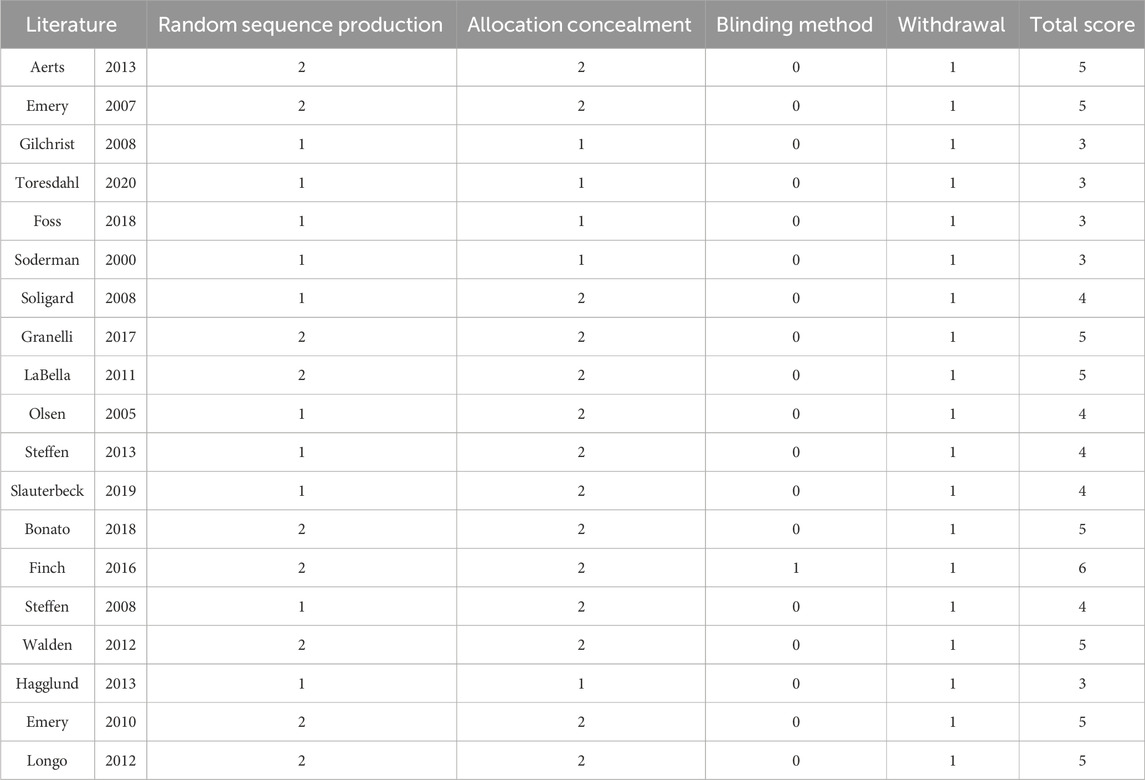
Table 2. Distribution of modified JADAD scale scores across included studies.
Overall effect testA total of 28,176 participants from the 19 included RCT articles were included in the overall effect test (see Figure 4). The results showed an effect size of RR = 0.75 (95% CI: 0.65–0.85; Z = 4.32; P < 0.00001), indicating that exercise interventions can effectively prevent lower limb knee injuries in young athletes. Due to I2 = 65% and P < 0.0001, a test for heterogeneity among the included studies was conducted, revealing moderate heterogeneity among the studies. Therefore, a random-effects model was used.
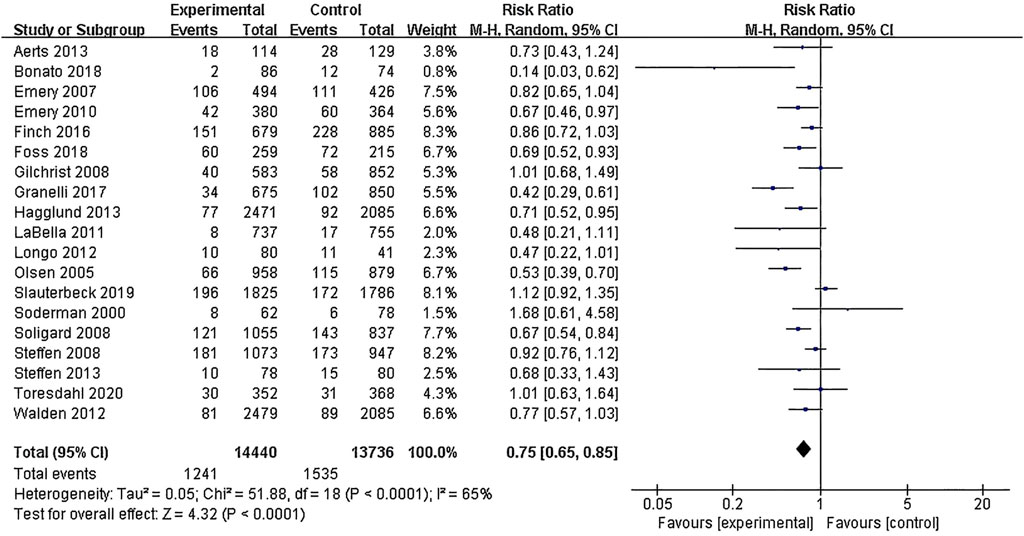
Figure 4. Forest plot of the overall effect test.
Sensitivity analysisSensitivity analysis was conducted on the 19 included articles by varying the effect size and excluding articles one by one. It was found that two articles contributed to high heterogeneity, and two articles contributed to moderate heterogeneity. By comparing them with other studies, it was discovered that one article had excessively long exercise duration of 30 min, while the other two articles combined injury results from stratified experimental groups. One of these articles involved interventions on handball athletes, indicating that the experimental design applied to the participants was the source of moderate heterogeneity among the studies. After removing these articles, the heterogeneity among the studies decreased to I2 = 12%. Comparing the effect sizes with and without the excluded article, the RR values remained within the original confidence interval, indicating a higher level of credibility for the meta-analysis results. Thus, these four studies can be retained.
Subgroup analysis results(1) Exercise Intervention Programs: Subgroup analysis including 28,176 participants from the 19 RCT showed low heterogeneity within the neuromuscular training group (I2 = 29%) and high heterogeneity within the comprehensive training group (I2 = 84%). Both groups demonstrated statistically significant reductions in risk, with the neuromuscular training group showing a more pronounced effect size: RR = 0.76 (95% CI: 0.68–0.85; Z = 4.80; P < 0.00001).The core strength training group (P = 0.96) and balance training group (P = 0.19) had insufficient sample sizes, thus no statistical significance was observed (Figure 5; Table 3).
(2) Exercise Duration: Subgroup analysis involving 26,612 participants from 18 RCT was conducted. The results showed low heterogeneity within the 5–15 min group (I2 = 0%) and high heterogeneity within the 16–30 min group (I2 = 76%). Both the 5–15 min (P = 0.001) and 16–30 min (P < 0.001) groups showed statistically significant effect sizes. The 5–15 min group had a more pronounced effect size with RR = 0.76 (95% CI: 0.65–0.90; Z = 3.30; P = 0.001) and lower heterogeneity within the group (Figure 6).
(3) Exercise Frequency: In a subgroup analysis encompassing 26,684 participants from 18 RCT, there was observed moderate heterogeneity between the 2–3 times per week group and the other week group (I2 = 60.9%), with both groups showing moderate heterogeneity internally. Both the 2–3 times per week group and varying weekly frequencies group had statistically significant effect sizes (P < 0.001). Notably, the group with varied weekly frequencies exhibited a more substantial effect size, with RR = 0.73 (95% CI: 0.66–0.82; Z = 5.50; P < 0.00001), indicating a more pronounced reduction in risk (Figure 7).
(4) Exercise Period: Subgroup analysis including 28,176 participants from 19 RCT was conducted. The analysis identified high heterogeneity when comparing the group with exercise periods of 26 weeks or less to the group with periods exceeding 26 weeks, as indicated by an I2 of 83.6%. Despite the high heterogeneity, both duration groups exhibited statistically significant effect sizes (P < 0.001). The group with exercise periods longer than 26 weeks demonstrated a more substantial effect, with RR = 0.72 (95% CI: 0.65–0.79; Z = 6.54; P < 0.00001), suggesting a more pronounced reduction in risk associated with longer exercise periods (Figure 8).
(5) Sample Size: Subgroup analysis including 28,176 participants from 19 RCT articles showed low heterogeneity within the group of studies with sample sizes ranging from 20 to 1,000 participants (I2 = 32%). Conversely, high heterogeneity was present in the group with sample sizes above 1,000 participants (I2 = 77%). Despite the differing levels of heterogeneity, statistically significant effect sizes were found in both groups (P < 0.001). The group with 20–1,000 participants exhibited a more pronounced effect size, with RR = 0.75 (95% CI: 0.65–0.86; Z = 4.10; P < 0.0001), indicating a substantial reduction in risk within this range of sample sizes (Figure 9).
(6) Gender: Subgroup analysis involving 20,101 participants from 13 RCT indicated moderate heterogeneity within the female group (I2 = 45%) and high heterogeneity within the male group (I2 = 85%). Both groups showed statistically significant effect sizes (P < 0.001). The male group showed a more pronounced effect size, with RR = 0.71 (95% CI: 0.61–0.83; Z = 4.21; P < 0.00001) (Figure 10).
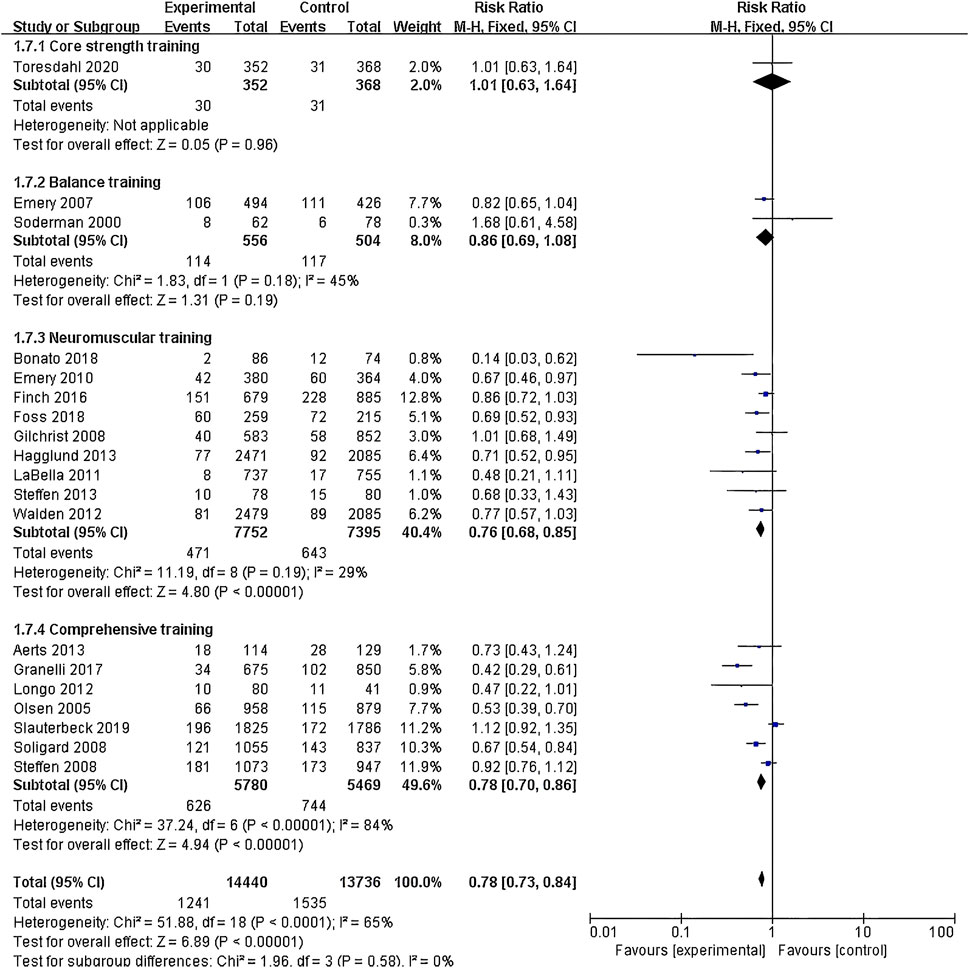
Figure 5. Forest plot of risk ratio by exercise intervention programs subgroup analysis.
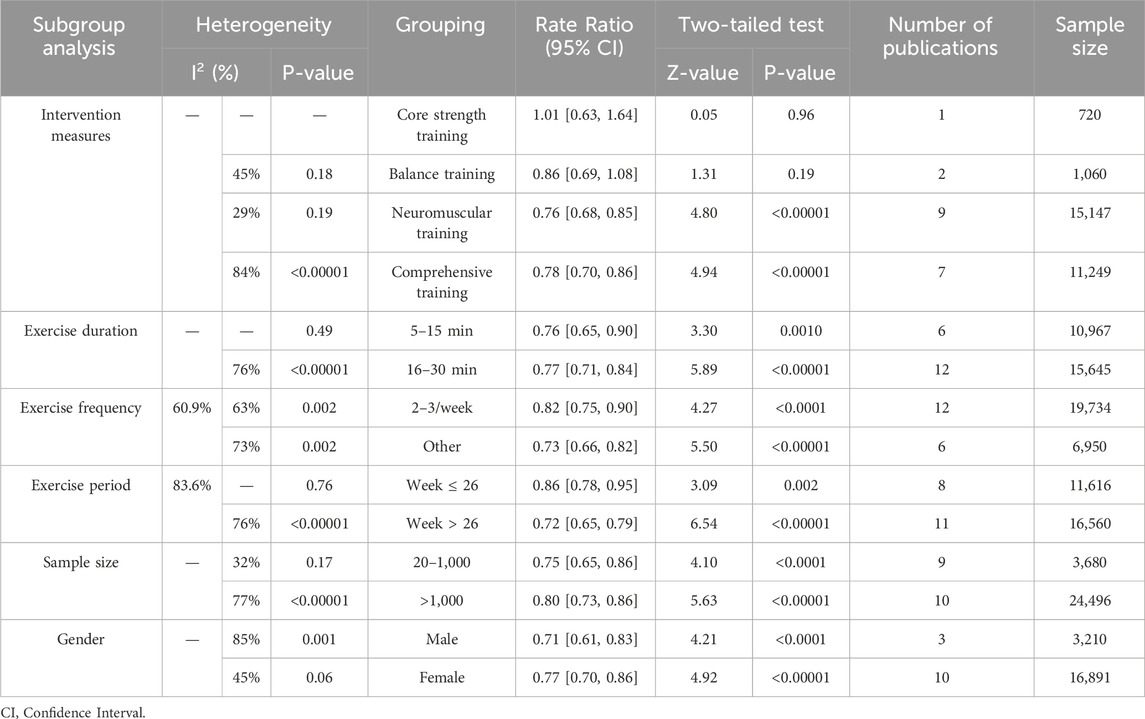
Table 3. Summary of subgroup analysis results.
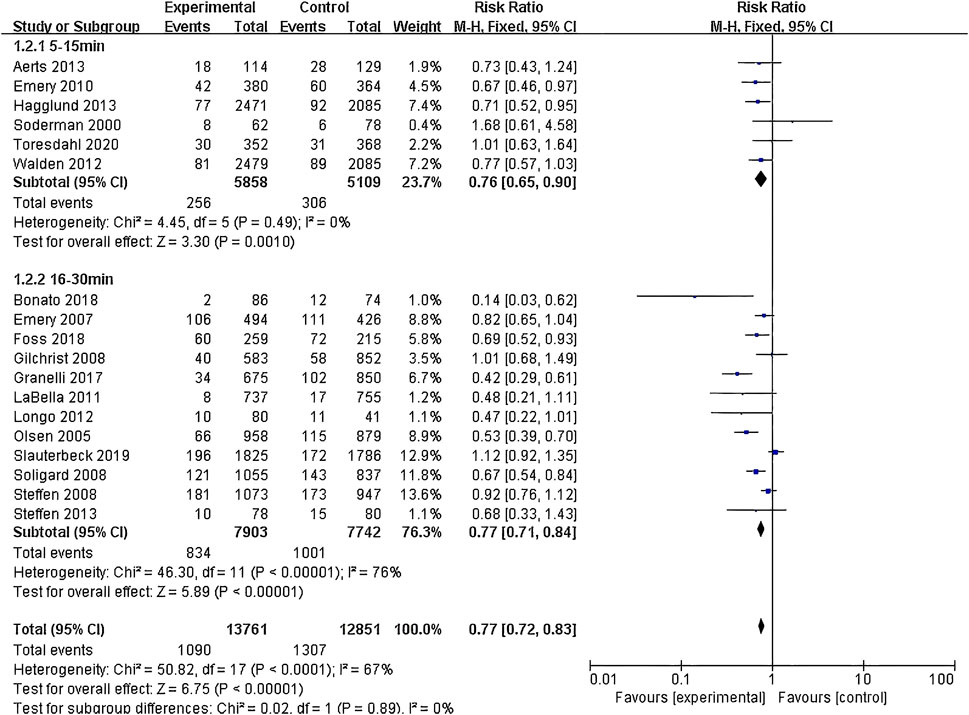
Figure 6. Forest plot of risk ratio by exercise duration subgroup analysis.
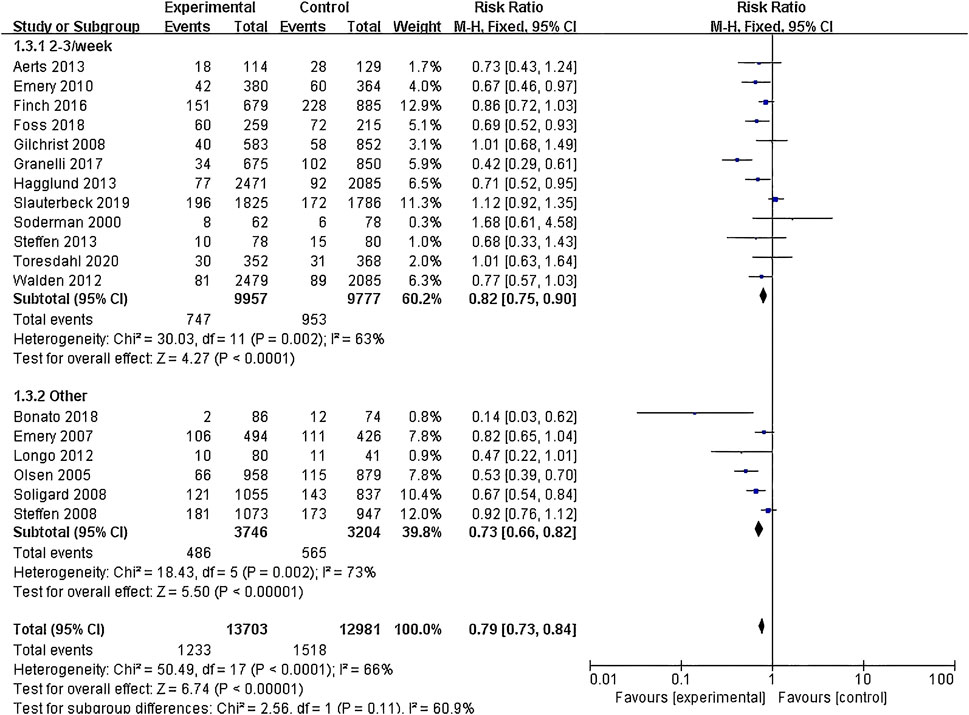
Figure 7. Forest plot of risk ratio by exercise frequency subgroup analysis.
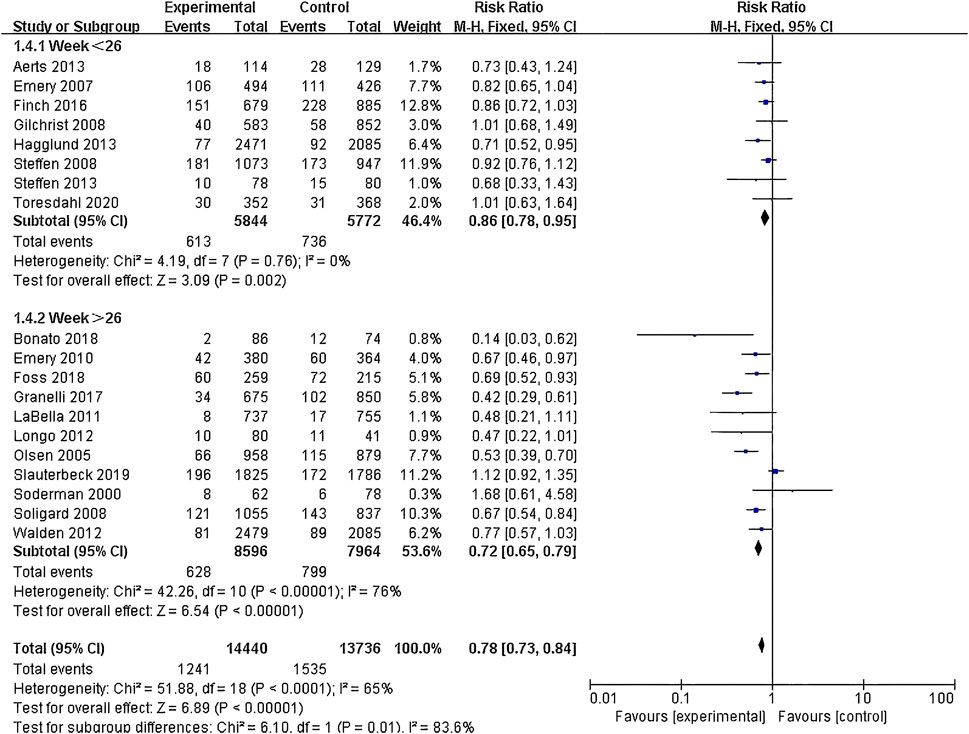
Figure 8. Forest plot of risk ratio by exercise period subgroup analysis.
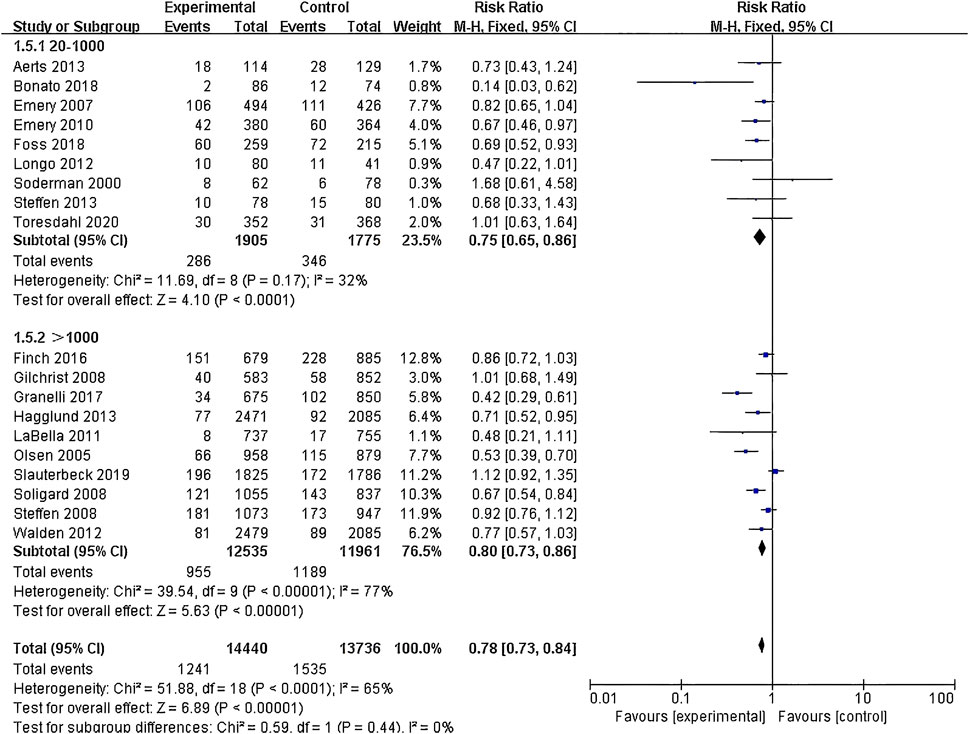
Figure 9. Forest plot of risk ratio by sample size subgroup analysis.
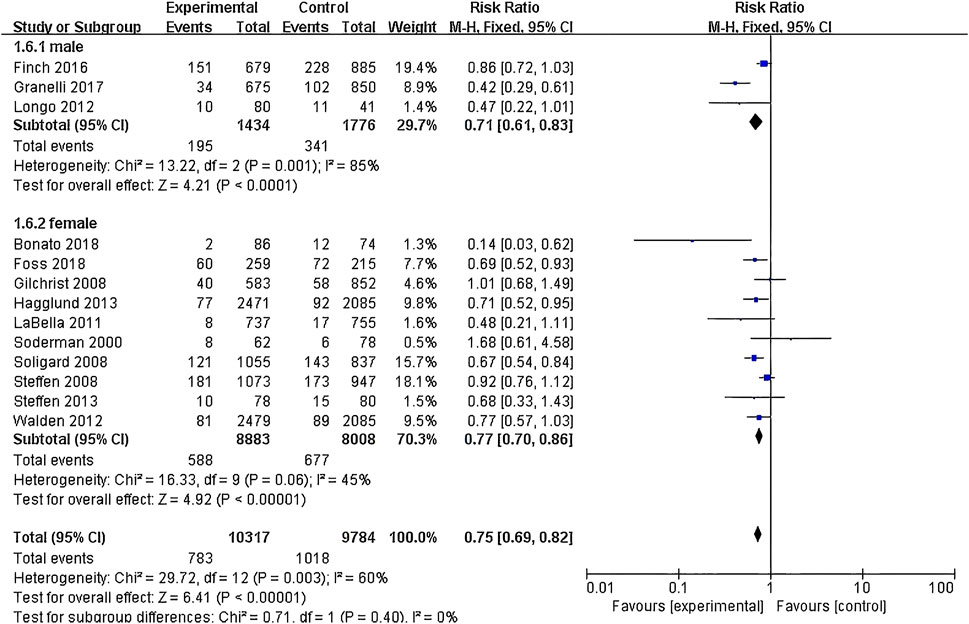
Figure 10. Forest plot of risk ratio by gender subgroup analysis.
Publication bias assessmentThe publication bias assessment was conducted using a funnel plot to evaluate the effect of publication bias on the meta-analysis of the preventive effect of exercise intervention on lower limb injuries (Figure 11). The plot revealed a primarily symmetrical distribution of data points around the central axis, with most points clustered above the line. There were only two articles were dispersed below the line, indicating potential bias compared to other studies. The symmetry observed in the funnel plot generally indicates an absence of significant publication bias within the study sample, lending credence to the reliability of meta-analysis outcomes.
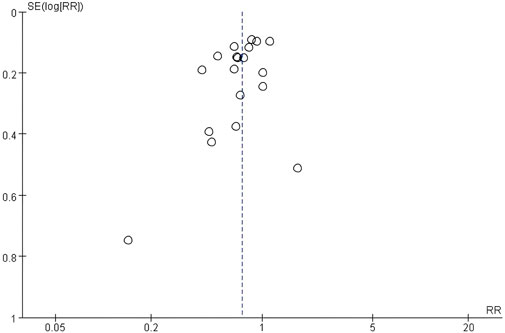
Figure 11. Funnel plot.
DiscussionIn this study, we conducted a meta-analysis of 19 RCTs to assess the effectiveness of exercise interventions in preventing lower limb knee injuries. The quantitative synthesis indicated that exercise interventions were effective in preventing lower limb knee injuries, with a pooled effect size (RR) of 0.75 (95% CI: 0.65–0.85; P < 0.001). Sensitivity analysis and subgroup analysis were performed on the included 19 studies to explore heterogeneity and identify the optimal intervention content, exercise duration, frequency, and period. The subgroup analysis of exercise intervention content revealed that all four intervention content types showed significant preventive effects on injuries. Previous studies have shown that core strength training can prevent ACL injuries by increasing the co-activation ratio of the hamstring and quadriceps muscles and reducing knee valgus and hip adduction angles (Jeong et al., 2021). Neuromuscular training, on the other hand, reduces the risk of sports-related injuries not only by increasing muscle strength and power but also by improving balance, speed, and agility (Zemková and Hamar, 2018). The intervention in the included neuromuscular training studies emphasized strength, agility, and balance, with a particular focus on plyometric exercises within the intervention, which were shown to significantly enhance voluntary motor control, awareness, and neuromuscular coordination. These characteristics distinguish neuromuscular training from isolated core strength training and balance training. Due to the limited sample size of core strength and balance interventions, no significant differences were observed. However, neuromuscular training intervention showed the best effect size (RR = 0.76; P < 0.001). Studies on different sports have indicated that exercise can enhance lower limb neuromuscular control, balance, muscle strength, and core strength, leading to the prevention of knee injuries. The occurrence of lower limb injuries is often associated with weak lower limb neuromuscular control, decreased balance, and insufficient core strength. Existing literature suggests that exercise-based prevention of lower limb knee injuries may be related to the improvement of these three factors (Akerlund et al., 2020; Andrew et al., 2013; Bulow et al., 2021; Jeong et al., 2021; Liu et al., 2016). Human movement not only involves mechanical structures but also requires a coordinated interplay between balance, neural control, and core strength. While it is important to examine the individual factors influencing knee injuries, it is also crucial to focus on their interrelationships. Core strength can improve the dynamic balance and coordination of the lower and upper limbs, thus reducing the risk of injury by maintaining the correct knee joint alignment (Affandi et al., 2019).
Enhanced balance, proprioception, and neuromuscular control may be associated with the prevention of lower limb knee injuries. A study involving 14 ACL-injured athletes examined the lower limb forward reach and three-dimensional force plate vertical jump tests after 3 and 6 months of rehabilitation treatment. The results showed that ACL injuries decreased the forward reach distance, peak jump and landing forces, and increased bilateral asymmetry, indicating that balance and strength were factors contributing to abnormal movement patterns (Dai et al., 2021). Muscle strength and balance are also correlated (Song et al., 2021). Hu conducted further research and found that lower limb strength is associated with dynamic postural stability. Improving dynamic postural stability through lower limb muscle strength training may reduce the risk of ACL injuries in the knee joint (Hu C. et al., 2023). The decline in neuromuscular control is also accompanied by changes in the structure of the lower limb knee joint, as reflected in the dynamic adaptation of the knee joint towards valgus alignment, which poses a significant risk for knee injuries (D’Onofrio et al., 2023). Following training interventions focused on balance and proprioception, rugby players experienced a 50% reduction in the occurrence of lower limb knee injuries (Attwood et al., 2018). A randomized controlled trial confirmed that specialized balance training in soccer could lower the incidence of hamstring and tendon injuries (Correia et al., 2020). This effect may be achieved by enhancing sensory input or accelerating neural conduction through balance and proprioception training, thereby improving the function and coordination of muscle-tendon units to better adapt to the upcoming exercise intensity. Furthermore, attention should be paid to muscle activation balance, as muscle imbalances are often reflected in significant differences in electromyography values. Earl’s study, which conducted electromyographic testing of six lower limb muscles during Y-balance exercises, demonstrated different activation patterns for muscles in different directions. Inner and inner posterior exercises can strengthen the quadriceps and help improve knee joint stability and ACL injury rehabilitation (Earl and Hertel, 2001). In addition to improving lower limb muscle balance, exercise can also increase hamstring muscle strength, optimize knee joint angles, and enhance posterior chain muscle strength, thereby improving the stability of the lower limb knee joint (Krommes et al., 2021).
The core strength is crucial throughout the entire process of body movement, transmitting upper and lower limb forces and regulating proper positioning of the center of gravity during exercise. Sasaki found that 8-week of continuous core muscle training can prevent lower limb injuries. This type of training can enhance athletes’ stability and control, reduce knee joint valgus torque, trunk flexion, and lateral inclination angles, and improve core strength, which is beneficial for preventing lower limb and exercise-related injuries, thus reducing biomechanical loads on the lower limbs and trunk (Sasaki et al., 2019). Guo found that dynamic core flexion strength can enhance countermovement jump height through arm swing, thereby improving athletic performance (Guo et al., 2020). Meanwhile, in terms of sports injuries, core stability plays a crucial role in preventing knee injuries during drop-jump landings (Guo et al., 2021). Training core strength and activating abdominal muscles effectively prevent lower limb injuries, especially non-contact ACL injuries. These methods improve neuromuscular control, reduce hip adduction angle and trunk lateral displacement, and reduce the risk of ACL injuries (Linde et al., 2018). Core strength training also enhances the trunk’s ability to resist perturbations, thereby reducing ACL load variables (Song et al., 2023). Saki concluded through an 8-week training that core strength training can improve kinematic characteristics, reduce high-risk landing mechanics, and prevent primary ACL injuries. It is recommended to perform core stability training after completing the postoperative rehabilitation plan to reduce the risk of re-injury (Saki et al., 2023). Therefore, by designing the content of core strength training during exercise, it is possible to improve the biomechanical structure of the lower limbs, enhance control over the lower limbs, and subsequently enhance control over the knee joint.
This study conducted subgroup analysis on exercise duration and found that both short durations of 5–15 min and moderate durations of 16–30 min can achieve the effect of preventing lower limb injuries. This is more feasible for various team sports and can be incorporated as warm-up exercises before different specialized training arrangements during the preseason or in-season. The study found that a short duration of 5–15 min achieved a better effect size (RR = 0.76; P = 0.001), providing the best preventive effect on lower limb sports injuries. This is consistent with the meta-analysis by Steib et al. (2017) on dose-response of neuromuscular training in preventing injuries in adolescent athletes, where a short duration of 10–15 min showed a better effect size than a moderate duration, consistent with the results of this study. On the one hand, this may be due to neuromuscular factors, and on the other hand, additional exercise interventions may increase the risk of knee joint injuries, as confirmed by the study by Savage et al. (2018), which showed that longer exercise durations lead to fatigue and increased knee joint flexion-extension torque, thereby increasing the risk of injuries.
Subgroup analysis of exercise frequency showed that interventions conducted in alternate weeks (4–5 times/week) had the greatest effect size in preventing lower limb knee joint injuries (RR = 0.73; P < 0.001). This may be because the exercise intervention serves as a warm-up before formal training, and a higher frequency of short-duration exercise interventions is needed to achieve the desired preventive effect on knee injuries. This is consistent with the study by Emery et al. (2022), which introduced neuromuscular training warm-up programs for basketball players and reduced their knee injury rate by 36%. A frequency of 4–5 times/week in exercise intervention can enhance neuromuscular control and increase lower limb muscle control, leading to injury prevention effects. In this study, the subgroup of exercise frequency at 4–5 times/week had high heterogeneity within the group, and only 6 studies were included. Further research on exercise frequency is needed in the future.
This study examines the impact of exercise duration on the relationship between exercise interventions and the prevention of lower limb knee injuries. Subgroup analysis based on exercise duration reveals that exercise interventions lasting more than 26 weeks yield a superior effect size (R = 0.72; P < 0.001). Consistent with previous research by Hu S. et al. (2023), this study demonstrates that exercise plans with a duration of 21–30 weeks in interventions targeting the hamstring muscles are more effective in injury prevention. The current results indicate that exercise interventions exceeding 26 weeks produce the optimal effects in preventing lower limb injuries. This outcome may be attributed to the optimization of neuromuscular control, balance, lower limb biomechanics, and core strength achieved through the 4–6-month lower limb injury prevention program.
Furthermore, subgroup analysis based on sample size indicates that the optimal effect size (RR = 0.75; P < 0.001) is achieved with sample sizes ranging from 20 to 1,000 subjects. This finding suggests that sample sizes within this range are more conducive to implementing intervention plans, as they result in relatively smaller data and measurement errors and lower within-group heterogeneity. Consequently, the results are more reliable, particularly in the context of group sports projects.
Female athletes are more predisposed to a higher risk of ACL injuries due to improper movement patterns (Ogasawara et al., 2024). Gender differences not only manifest in sports injuries but also impact the relationship between exercise interventions and lower limb knee injuries. Studies have demonstrated that exercise interventions effectively reduce non-contact anterior cruciate ligament injuries in female athletes (Mattu et al., 2022). However, subgroup analysis focusing on gender reveals that exercise interventions have a better effect size in preventing lower limb knee injuries in males (RR = 0.71; P < 0.001). This finding may be attributed to the limited number of male-specific studies (3 articles) compared to female-specific studies (10 articles) in this subgroup analysis, along with the higher heterogeneity within the male group. Future research should strive to include more high-quality literature to investigate the effects of exercise interventions on different genders.
Limitations and future perspectivesLimited research on high-level adult athletes: Currently, studies on exercise interventions primarily focus on adolescent athletes in middle and high school (12–20 years old), while there is a lack of research on adult athletes involved in elite competitions. Considering the higher incidence of knee joint injuries in high-level competitive sports, investigating the effects of exercise interventions on high-level athletes would be of significant importance. Therefore, future studies should aim to include high-level adult athletes in their research.
Lack of standardized exercise protocols: There is currently no consensus on the specific design of exercise programs for lower limb injury prevention. Different sports may have varying training content and sequencing, making it difficult to determine which factors contribute most significantly to preventing knee injuries. The diversity in intervention content also complicates the interpretation of physiological mechanisms. Future research could incorporate neurophysiological and proprioceptive aspects to further investigate the underlying mechanisms. Additionally, quantitative analysis of exercise intensity and load, as well as the resulting metabolic stress on the body, should be conducted to better understand the effectiveness of lower limb injury prevention.
Biomechanical variations among different sports: The emphasis of exercise interventions may differ across various sports, which could introduce bias in the interpretation of biomechanical structures. Future studies should explore the characteristics of intervention content specific to each sport to gain a better understanding of their effects on injury prevention.
Insufficient inclusion of high-quality literature: The limited number of high-quality studies included in the analysis may contribute to heterogeneity among studies. Therefore, future research should prioritize high-quality studies to enhance the reliability of findings regarding the effectiveness of exercise interventions.
ConclusionWe advocate for the integration of neuromuscular training into programs designed to prevent lower limb knee injuries. This approach is identified as a foundational strategy in ensuring knee health. The efficacy of such programs is maximized when they include exercises lasting 5–15 min, conducted 4–5 times per week, over a period extending beyond 26 weeks. This regimen not only offers a practical solution but also stands as an effective method to significantly lower the incidence of knee injuries. By adopting this evidence-based protocol, practitioners can better safeguard the knee health of athletes and individuals engaged in physical activities, ensuring long-term musculoskeletal wellbeing.
Data availability statementThe original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Author contributionsGZ: Writing–original draft, Writing–review and editing. SZ: Data curation, Writing–review and editing. TL: Investigation, Writing–review and editing. LG: Supervision, Validation, Writing–review and editing. LL: Supervision, Writing–review and editing.
FundingThe author(s) declare that financial support was received for the research, authorship, and/or publication of this article. We acknowledge the financial support from the construction project of the 2025 Industry Science and Technology Collaborative Innovation Center (SL2024B04J00048) provided by Guangzhou Science and Technology Bureau, as well as the 2024–2025 Science and Technology Innovation and Sports Culture Development Project provided by Guangdong Provincial Sports Bureau (GDSS2024N029).
Conflict of interestThe authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s noteAll claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary materialThe Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fphys.2025.1455055/full#supplementary-material
ReferencesAerts I., Cumps E., Verhagen E., Mathieu N., Van Schuerbeeck S., Meeusen R. (2013). A 3-month jump-landing training program: a feasibility study using the RE-AIM framework. J. Athl. Train. 48 (3), 296–305. doi:10.4085/1062-6050-48.3.18
PubMed Abstract | CrossRef Full Text | Google Scholar
Affandi N. F., Mail M. S. Z., Azhar N. M., Shaharudin S. (2019). Relationships between core strength, dynamic balance and knee valgus during single leg squat in male junior athletes. Sains Malays. 48 (10), 2177–2183. doi:10.17576/jsm-2019-4810-13
CrossRef Full Text | Google Scholar
Akerlund I., Walden M., Sonesson S., Hagglund M. (2020). Forty-five per cent lower acute injury incidence but no effect on overuse injury prevalence in youth floorball players (aged 12-17 years) who used an injury prevention exercise programme: two-armed parallel-group cluster randomised controlled trial. Br. J. Sports Med., 54(17), 1028–1035. doi:10.1136/bjsports-2019-101295
PubMed Abstract | CrossRef Full Text | Google Scholar
Andrew N., Gabbe B. J., Cook J., Lloyd D. G., Donnelly C. J., Nash C., et al. (2013). Could targeted exercise programmes prevent lower limb injury in community Australian football? Sports Med. 43 (8), 751–763. doi:10.1007/s40279-013-0056-7
PubMed Abstract | CrossRef Full Text | Google Scholar
Attwood M. J., Roberts S. P., Trewartha G., England M. E., Stokes K. A. (2018). Efficacy of a movement control injury prevention programme in adult men’s community rugby union: a cluster randomised controlled trial. Br. J. Sports Med., 52(6), 368–374. doi:10.1136/bjsports-2017-098005
PubMed Abstract | CrossRef Full Text | Google Scholar
Bonato M., Benis R., La Torre A. (2018). Neuromuscular training reduces lower limb injuries in elite female basketball players. A cluster randomized controlled trial. Scand. J. Med. and Sci. Sports 28 (4), 1451–1460. doi:10.1111/sms.13034
PubMed Abstract | CrossRef Full Text | Google Scholar
Bulow A., Bellemare A., Anderson J. E., Leiter J. R. S., MacDonald P. B., Peeler J. D. (2021). Lower extremity kinematics of the Y-balance test in healthy and ACL injured adolescent females. Int. J. Sports Phys. Ther. 16 (2), 38
Comments (0)